The Covid Collaborators | Brave New Real-World Data by Maddie Bannon
"The Covid Collaborators" is an investigative series by Maddie Bannon that was originally published on James Jordan's Manufacturing Reality. Visit and support his work at ManufacturingReality.org.
“All right then,” said the savage defiantly, I’m claiming the right to be unhappy.”
“Not to mention the right to grow old and ugly and impotent; the right to have syphilis and cancer; the right to have too little to eat, the right to be lousy; the right to live in constant apprehension of what may happen tomorrow; the right to catch typhoid; the right to be tortured by unspeakable pains of every kind.”
Dr. Robert Califf is a cardiologist from North Carolina who made a name for himself by organizing and overseeing massive clinical trials in the early 1990s. His most famous work includes the 1993 GUSTO trial, an international randomized trial populated by over 40,000 subjects investigating four different treatments for myocardial infarction (heart attacks).1 This landmark trial was performed early on in his thirty year tenure at Duke University. There, he has served as a professor of both medicine and cardiology, and remains a practicing cardiologist. His colleagues at Duke adulate him, praising him for being “a visionary committed to ensuring the safety and health of our global community.”2 He is among the ten most frequently cited authors in biomedical science, having written over 1,200 peer-reviewed papers during his academic career.
However, as with many prominent health “experts,” Dr. Califf’s pharmaceutical and biotechnology corporation ties are abundant. For instance, the GUSTO trial was funded by a handful of private pharmaceutical companies including Bayer and Sanofi.3 Many of his 1,200+ academic papers are punctuated with disclosure statements that read like this one:
Dr Califf receives support from the National Institutes of Health and the Patient-Centered Outcomes Research Institute. Dr Califf also receives grant support from Amylin, Novartis, Eli Lilly and Co, Schering-Plough Research Institute, Johnson & Johnson/Scios, Aterovax, and Bayer; grants and personal fees from Bristol-Myers Squibb, Janssen Research & Development, Merck, and Roche; and personal fees from Genentech, GlaxoSmithKline, Heart.org/Daiichi Sankyo, Kowa, Servier, Medscape, The Medicines Company, Pfizer, Gambro, Gilead, DSI-Lilly, CV Sight, Heart.org/Bayer, Bayer Pharma AG, Bayer Healthcare, Parkview Health, Pozen, Orexigen, Nile Pharma, and WebMD. Dr Califf holds equity in N30 Pharma, Portola, and Nitrox LLC.4
So, when he was nominated for a position at the Food and Drug Administration (FDA) in 2015, Califf was met with tremendous pushback.5 Bernie Sanders (I-VT) resisted his nomination citing his vast pharmaceutical financial obligations and pointing to his involvement in the revolving door between the FDA and those private companies.6
The already cozy connection between one of his main projects, Duke Clinical Research Institute (DCRI), and the FDA was highlighted in the mainstream media as odd and inappropriate since the trials conducted at DCRI were controversial in nature and favorable to the drug industry (as they remain today).7 These kinds of conflicts of interest, however, did not prevent him from being confirmed as the Deputy Commissioner for FDA’s Medical Products and Tobacco division or, in 2016, as the FDA Commissioner.
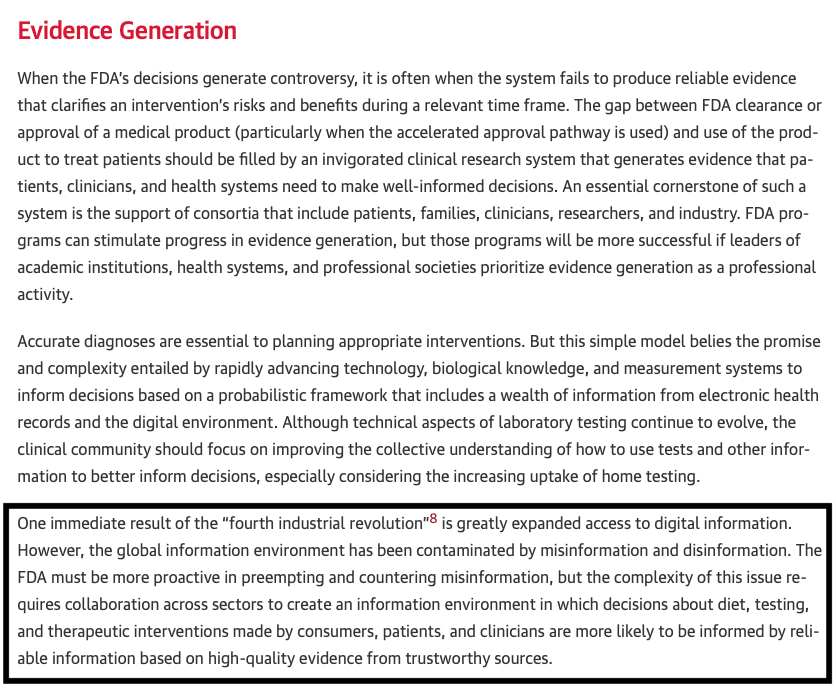
In reports and interviews, Dr. Robert Califf comes across as an ordinary southern man in his seventies who makes occasional jokes and supports his local college football team. He wears a charming smile and is often pictured in jeans and a button-up shirt, rather than the typical three-piece suit uniform worn by doctors and bureaucrats. Behind the disarming exterior, though, is a striking ideology. Califf is a devout Fourth Industrial Revolution (4IR)8 evangelist and true believer.
In his academic papers,9 Califf often glowingly cites Klaus Schwab and his global-technocratic cause and enthusiastically argues in favor of converging biology with technology at an accelerated rate. His non-academic efforts include convincing people like then President Barack Obama that the 4IR is happening whether we like it or not.10 “Getting that right was the most important thing in the future of the American economy and its health,” Califf describes, “[Obama] knew that the current FDA paradigm was not suited and something different had to be done.”11
Snippet from Califf’s August 2022 Paper published on Jama Network
The latter half of Califf’s career has been spent, at least in part, in this pursuit, tirelessly dedicated to the task of removing the obstacles facing the 4IR. Before touching on Califf’s endeavors in this regard, we will take a closer look at what the 4IR entails for the public health sphere.
The Fourth Industrial Revolution is the brain child of Klaus Schwab, the founder of the World Economic Forum (WEF). He describes it as an inevitable “convergence of digital, biological, and physical innovations,” that will, “profoundly transform institutions, industries, and individuals.”12 Among other overtly technophilic ideas about the future, Schwab conceives of a world saturated with artificial intelligence (AI). Omnipresent sensors that communicate with AI will seamlessly and instantaneously harvest your unlocked biological data to identify pharmaceutical market gaps so that clinical trials can be performed in the “real world,” without your knowledge or consent, rather than in a traditional clinical setting. The era of slow and costly clinical trials needs to end now, he seems to be arguing, as it is inhibiting drug and medical device companies from developing marketable, transformative products at a satisfactorily rapid rate.
Instead of focusing so narrowly on questions of safety and efficacy,13 all of our biological and behavioral data, as made one with digital innovations, ought to be freed from data silos, standardized, and made available to researchers so that clinical trials can be run in parallel to the introduction of those drugs and medical devices in the market. All of us, wittingly or not, will be remade into our “quantified selves” so that we may serve as uncompensated and unprotected clinical trial subjects. As though they do not already have plenty of incentives, this would provide the drug and medical device manufacturers a reason to develop innovative medical products at a record pace and profit exorbitantly off of those remain the market (i.e. do not cause significant harm to consumers and get recalled). Novel clinical trials will be designed and performed based on this “real-world data” generated by people and the environment.
Whether by monitoring you through your physically integrated biosensors, through sensors quietly placed in our wastewater systems, or by some other means, Schwab predicts that governments will “increase their control over populations, based on pervasive surveillance and the ability to control digital infrastructure.”
Privacy concerns aside, he would like you to be convinced that this is a desirable outcome because the world is dangerous and safety is worth the cost. Autonomous and biological weapons are becoming easier for individuals and small groups to use and potentially cause “mass harm.” Such surveillance and “real-world” clinical trials will help governments become more agile in their regulation and medical countermeasure (MCM) development. Strictly for defensive purposes, of course.
Right man, right job, right time
In significant ways, Califf’s life work supports some aspects of Schwab’s vision. A few years after the completion of the GUSTO trial, he became the founding director of the Duke Clinical Research Institute (DCRI).14 The DCRI performs multinational clinical research trials, “megatrials” (>5,000 participants), offers trial support programs, conducts medical device trials, and implements research into medical services at the Duke University School of Medicine. DCRI also partners with technology companies to provide a clinical research platform for mobile phone applications and wearable devices like smart watches. More than half of the funding for DCRI comes from the drug industry and, in 2019, was in the top ten in the nation for medical research funding from the National Institutes of Health.15
In 2007, the DCRI became the host of the Clinical Trials Transformation Initiative (CTTI) self-described as “a public-private partnership designed to create new solutions for better, more efficient clinical trials.”16 The CTTI was co-founded by the FDA in partnership with Duke and operates with a heavy emphasis on using “real world evidence,” electronic health records (EHRs), and digital health trials. The CTTI’s apparent objective is to cut down on the amount of money and time it takes to figure out if a drug or medical device is safe for use and effective at achieving its purpose. Furthermore, CTTI hopes to “maximally leverage available clinical and nonclinical data, including data collected via digital technologies, to minimize collection of necessary trial specific data.”17 Funding for CTTI comes from the FDA and the many tendentious “member organizations” pictured below:
A few major obstacles stand in the way of CTTI’s vision for faster and cheaper clinical trials, however. The first, and most important, obstacle is to overcome the exclusive reliance on the gold-standard randomized clinical trial model. Randomized clinical trials (RCTs) have become central in medical research because they stubbornly and ardently control for all variables. A participant either receives the medical intervention or a placebo and results are derived solely from variation of this condition with all other conditions being, as much as is possible, the same across all participants. Thus, if the participants receiving the intervention have better health outcomes than those receiving the placebo, you can be confident that your intervention works. What CTTI seeks to do, however, is to use “real-world evidence” in place of evidence generated by RCTs.
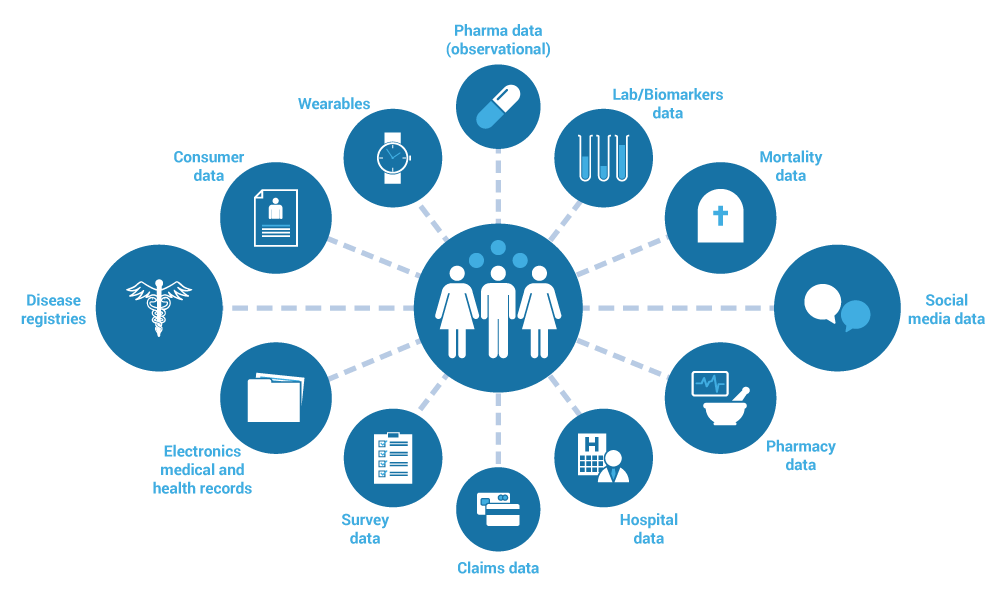
What counts as “real-world data.” Graphic courtesy of CHCUK
Real-world evidence (RWE) is defined by the FDA as “the clinical evidence regarding the usage and potential benefits or risks of a medical product derived from analysis of real-world data” where real-world data (RWD) is defined as “data relating to patient health status and/or the delivery of health care routinely collected provided [sic] outside of a research setting.”18RWD is collected from a vast array of sources including electronic health records (EHRs) submitted by medical professionals during a doctor or hospital visit, insurance claims and billing data, medical product and disease registries, the patient themselves (e.g. data submitted through an app), wearable devices, cellphones, and social media.
It is easy to imagine how evidence generated from these sources might come at a much lower cost than that derived from RCTs. Participants do not need to be compensated for their time, medical staff do not need to be hired to administer the intervention/placebo or record observations, time does not need to be spent searching for participants who meet the trial criteria, and so on. However, cheaper trials come with their own costs.
RWE can be highly untrustworthy as it can be inaccurately measured and/or reported, and there are seemingly no feasible means by which to differentiate between high and low quality RWD. Furthermore, data collected by one source like an insurance provider or biller may not be “interoperable,” meaning it might be formatted in an entirely different way than another source like a mobile phone. Thus, some information may be lost in translation when reformatting the data.
On top of that, participants in the study must subject themselves to near constant surveillance, surrendering their location data, personal health information, and privacy online. This discourages participation, limits sample sizes, and homogenizes, at least to some degree, the population being studied. Admittedly, this last phenomenon only occurs when you have to ask people to enroll in a trial and give up their privacy. This is no longer needed in all cases.
21st Century Blurs
Regardless of the actual utility of trials based on RWE, Califf has done, and continues to do, everything in his power to force the regulatory agencies, the government, and the science communities to accept them as valid and incorporate their tenets into medical and bureaucratic practices. Califf and company made a giant leap forward in this effort when the 21st Century Cures Act was signed into law in late 2016 by then President Obama19 while Califf was occupying his first position at FDA as the deputy FDA Commissioner.
Obama signs the 21st Century Cures Act into Law 12/13/2016. Photo courtesy of SMART.
The stated purpose of the Cures Act, according to the FDA, is to “enhance our ability to modernize clinical trial designs, including the use of real-world evidence, and clinical outcome assessments, which will speed the development and review of novel medical products, including medical countermeasures,” and to “incorporate patient perspectives” into the development of pharmaceuticals and medical devices while they are being reviewed by the FDA.20 Califf, and a few of his colleagues at FDA, including the acting FDA Commissioner Dr. Stephen Ostroff, claim to have been solicited by those legislators drafting the bill to provide technical assistance, however the contents of the Cures Act seem to suggest otherwise.
When the Cures Act was initially proposed, it was met with condemnation by consumer advocates and ethics watchdogs. One article from the time reads, “the FDA’s Center for Devices and Radiological Health (CDRH) and AdvaMed ‘worked together on the proposed language for most of the device provisions in’ the Cures Act, according to an FDA memo seen by Bloomberg from an Aug. 7 meeting […] Robert Califf, who was recently nominated to lead the FDA, also attended the meeting, along with AdvaMed officials and execs from device giants Johnson & Johnson ($JNJ) and St. Jude Medical ($STJ).”21 Another article aptly points to the unprecedentedly perverted nature of the Cures Act drafting process, reading,
While industry has the right to lobby Congress directly, it is unseemly and unacceptable for the FDA to collaborate with regulated industries in drafting laws that would directly affect the regulatory oversight of those industries. No one from the FDA should have been involved in such a process, which violates the most elementary ethical standards. The last person who should have been collaborating with the industry over policy proposals is the person in line to run the agency. Yet Califf did exactly that in the August meeting.
Despite the reasonable backlash, the Cures Act was passed with bipartisan support and was signed into law later that same year.
TLDR
Lobbying this bill to members of Congress was not cheap, costing pharmaceutical and medical device companies around a half billion dollars. The proposals in the Cures Act are likewise expensive, and were funded in part by a sell off of 25 million barrels of crude oil from the strategic petroleum reserve over three years (2017-2019). Although many of the proposals contained in the massively long piece of legislation (who reads these things?) are worth serious scrutiny, including the Biden Cancer Moonshot Initiative and the BRAIN initiative,22 only a few of them are relevant to my purposes here.
To spare you the pain of a deep dive into a typically tepid, brain-sucking piece of legislation, I have condensed the relevant proposals and provisions into a list of seven main ideas. However, I would encourage everyone to look beyond the surface as far as you can tolerate.
Standardized EHRs for ease of transmissibility between entities.
Initialized a program to find a public-private or public-public universal EHR collection platform for use by medical professionals and consumers.
Waived informed consent requirements for “minimal risk” trials.
Incorporated RWE in trial design and fostered its use in other areas.
Established provisions for the use of Priority Review Vouchers for the development of Medical Countermeasures (MCM)23 against an identified material threat.
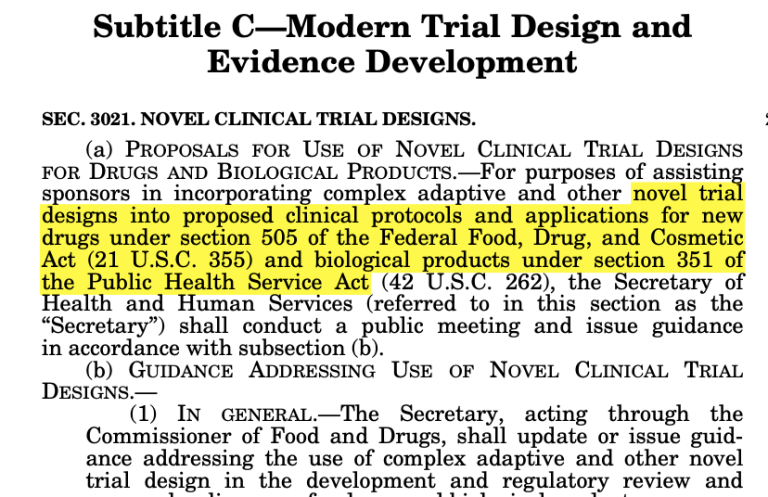
Side-stepped conventional regulatory measures by allowing for “novel trial designs” that allow for more rapid drug and medical device approval.
Emphasized the exploitation of genetic information in the Precision Medicine Initiative that has collected the genetic material and information of over one million Americans for research and trial purposes.
In sum, the 21st Century Cures Act served as a very important tool to ease regulations on patient data and clinical trials, allowing for clandestine surveillance on electronic health records and a reformulation of the idea of “safe and effective” drugs and medical devices. Medical data, which by the FDA’s definition includes genetic information, data collected from your phone, wearable devices, “implantables,” smart devices in your car or home, and social media, is more widely available to those interested in collecting it and is formatted in a way that makes it easier to be utilized for any suited purpose.24Medical treatments and devices are entering the market without being subjected to the typical rigors of a randomized clinical trial.
As you may recall, these effects are critical to the acceleration of the Fourth Industrial Revolution. In the short term, however, those who benefit are the information technology companies who compete over lucrative opportunities to build the systems that house and transfer your data, and the pharmaceutical and medical device companies that rush their products to market while making grandiose claims about their efficacy and safety. For instance, “novel trial designs” and RWE were utilized to make a press release from Pfizer in March 2021 regarding their mRNA jab (recipient of a priority review voucher from the FDA) possible, in which they state,
The Israel Ministry of Health (MoH), Pfizer Inc. and BioNTech SE today announced real-world evidence demonstrating dramatically lower incidence ratesof COVID-19 disease in individuals fully vaccinated with the Pfizer-BioNTech COVID-19 Vaccine (BNT162b2), underscoring the observed substantial public health impact of Israel’s nationwide immunization program. These new data build upon and confirm previously released data from the MoH demonstrating the vaccine’s effectiveness in preventing symptomatic SARS-CoV-2 infections, COVID-19 cases, hospitalizations, severe and critical hospitalizations, and deaths.25
Even though, a year later, billionaire philanthropist and COVID-19 vaccine advocate Bill Gates would admit that the mRNA jabs “do not protect you from getting infected.”26One statement is supported by RWE and one is supported by reality.
One Man’s Google is Another Man’s FDA
Califf left the FDA in 2017 and, a couple of years later, decided to pursue a career at Google/Alphabet as their head of health strategy and policy. He focused his work in their Verily Life Science offshoot that seeks to use patient generated data and wearable devices to produce medical insights in “precision health”.27 As the prolific Whitney Webb mentions in her article about Wellcome Leap and its undertakings, the words “precision health” are used as a “code phrase for treatments based on patients’ genetic data and/or for treatments that alter nucleic acid (e.g., DNA and RNA) function itself.”28
While at Google/Alphabet, Califf oversaw Project Baseline29 which, predictably, partnered with universities including his alma mater and employer, Duke University. Project Baseline’s primary aim was, and still is, to “map human health” by collecting data. They recruited at least ten thousand volunteers in 2017 and gave them proprietary “study watches” that would collect and transmit passively generated health, activity, and location data back to Verily.
The outcomes of Project Baseline are unclear. At least, in one blog posting, they proudly claim to have found evidence that “highlighted the effects of Daylight Savings Time on sleeping patterns – suggesting that ‘springing forward’ resulted in changes in our participants’ sleep quality, time, and restedness,”30 and that oral health is related to overall health. Simply groundbreaking.
Regardless of the wealth of new insights, or lack thereof, generated by his time spent working at Alphabet on Project Baseline, Califf certainly generated wealth for himself from the endeavor, totaling $2.7 million over the course of two years. Furthermore, he was granted $1-$5 million in equity in the company, which he still holds today as FDA Commissioner. Califf was recruited by President Biden in 2021 for the position at FDA, and was confirmed early this year despite his copious ties to pharmaceutical companies and sustained conflicts of interest. In his financial disclosure,31 he declares that he is still receiving compensation from Google/Alphabet as he is retaining his duties and position at Verily Life Sciences although his title has changed to “Science Advisor.”
Verily changed their mission statement shortly after Califf was confirmed to lead the FDA in 2022. It now reads “to bring the promise of precision health to everyone, every day.” In a blog post written by Verily’s current president and chief operating officer Stephen Gillett, he alludes to the Fourth Industrial Revolution, describing how a new era of information and technology is rapidly approaching32 that can transform medicine and all of us as individuals. In the candy-coated language of a salesman, we are pitched the transhumanist idealism of living longer lives, free of disability and disease, but what is the cost of this utopia?
Isn’t there something in living dangerously?
As we have seen, colossal entities like Alphabet, the FDA, and the WEF are apparently unified in their vision of creating an omnipotent and omnipresent surveillance mechanism that reaches beyond the walls of your home, into your bedroom, into your car, into your very genes, and seeks to use this information to sell you new, inadequately tested products for a healthy profit. At the same time, they expect you to offer up your data freely, to buy and swallow these products with fervent gratitude as you will be convinced doing so is necessary for your health and happiness in life. As Califf himself stated at a Talks at Google event,
“One thing you learn at the FDA, in a big way is that, when people are healthy, they really do behave like consumers. And that is very little risk tolerance, a lot of desire for independence, particularly in Americans […] but when people get sick, they get dependent quite quickly, they’re also willing to take more risks and they’re more vulnerable to people selling them things when they are atrisk.
Verily’s president and COO, in the same blog post mentioned above, asks himself the question, “why precision medicine now?” The answer he gives is this: “We are living in a time of massive increases in health information and computing power, combined with decreases in life expectancy, alarming and rising incidence of chronic diseases like diabetes, and increased demand for value-based care and improved outcomes. […] There are gaps in data, insights and incentives that all need to be addressed if we are to truly drive change and deliver on what we know is possible.” In other words, people are demoralized, sick, dependent, and willing to take risks. The infrastructure for the 4IR has been built and awaits use. We have a true believer in power at the world’s most trusted food and drug regulatory agency. Why now? Because the conditions, as they have designed them to be, are ideal.
Addendum
Added 12/4/2022
Since this installment was published in June, 2022, there have been a couple of notable developments.
First, in August, 2022, Duke Clinical Research Initiative (DCRI) — the big pharma friendly mega trial organization set up by FDA in partnership with Califf’s alma mater and employer, Duke University, as mentioned earlier — was handpicked by the NIH to coordinate the “NIH RECOVER Long Covid Initiative.” According to the NIH, there are over 200 symptoms of “long covid” that “may be different for everyone.” The symptoms may “come and go,” last a few weeks, months, or longer. With such a broad definition of “long covid” and a $1.15 billion budget, researchers at academic institutions will be conducting an observational study of 17,000+ children and adults for four years to learn more about “this new illness.”
According to the study protocol, a large part of the observation will be done through analyzing real-world data as described earlier. The study is set to begin in 2023, and the participants will be asked to provide biological material samples, however the majority of data will be harvested through self-reported questionnaires and EHRs.
Secondly, Cures 2.0, a bill designed to build on the law enacted by the 21st Century Cures Act, may be voted on by the House of Representatives in the near future. The draft was introduced in the House in November of 2021 and it was rumored to be facing a vote in Summer 2022, however it seems to have been punted to 2023.
If passed the bill would establish an ARPA-H, a health and medicine equivalent of the Defense Advanced Research Projects Agency (DARPA), designed to “to accelerate biomedical research and innovation through grants, contracts, cash prizes, and other means. The FDA may work with ARPA-H to expedite the development of medical products through specified activities.”34 In remarks to a joint session of Congress in April 2021, President Biden initially proposed this idea:
“Today, Mr. Secretary, that’s less than 1 percent. China and other countries are closing in fast. We have to develop and dominate the products and technologies of the future: advanced batteries, biotechnology, computer chips, clean energy.
The Secretary of Defense can tell you — and those of you on — who work on national security issues know — the Defense Department has an agency called DARPA — the Defense Advanced Research Project Agency. The people who set up before I came here — and that’s been a long time ago — to develop breakthroughs that enhance our national security -– that’s their only job. And it’s a semi-separate agency; it’s under the Defense Department. It’s led to everything from the discovery of the Internet to GPS and so much more that has enhanced our security.
The National Institute of Health — the NIH –- I believe, should create a similar Advanced Research Projects Agency for Health. (Applause.)
And that would — here’s what it would do. It would have a singular purpose: to develop breakthroughs to prevent, detect, and treat diseases like Alzheimer’s, diabetes, and cancer.”
While Biden is correct in asserting DARPA’s involvement in and contribution to the creation of beneficial technologies like the internet and GPS, DARPA has a long, blood-stained history of monstrous and tyrannical creations as well. These include the chemical defoliant Agent Orange used in Vietnam and the big brother-esque Total Information Awareness Program developed by John Poindexter, among many others. So, while a health version of DARPA may be an apt comparison, it does not necessarily bode well for the world.
In any case, The Milken Institute, which describes itself as “instrumental in gaining support for the 21st Century Cures Act in 2016,” lauded Cures 2.0 for its aim to facilitate “development of cell and gene therapies.”35
In addition, Cures 2.0 would modify the timeframe and require additional guidance relating to the approval of “breakthrough” drugs or other medical interventions. It would strengthen and further entrench the use and dependence on RWD and RWE for trial design and, of course, calls for more funding and work on “pandemic preparedness.”
Although no action is currently being taken on this legislation, it is certainly worth keeping an eye on.
Note: My writing is my opinion best representation of the news and publicly available information I find on the internet. I encourage my readers to do their own research and come to their own conclusions.
The Gusto Investigators. “An International Randomized Trial Comparing Four Thrombolytic Strategies for Acute Myocardial Infarction.” The New England Journal of Medicine. 2 September, 1993. https://www.nejm.org/doi/full/10.1056/nejm199309023291001
Califf, Robert M. “Improving Clinical Outcomes in the Era of Information Ubiquity.”Journal of the American Society of Nephrology. 30(1):p 7-12, January 2019. | DOI: 10.1681/ASN.2018111128.https://jasn.asnjournals.org/content/30/1/7
Real-World Evidence Generation and Evaluation of Therapeutics: Proceedings of a Workshop (2017) National Academies of Sciences, Engineering, and Medicine. 2017. Real-World Evidence Generation and Evaluation of Therapeutics: Proceedings of a Workshop. Washington, DC: The National Academies Press. Ch 2:p 7-86. https://doi.org/10.17226/24685. https://www.nap.edu/read/24685/chapter/3
Duke Clinical Research Institute. “Duke University among top 10 in nation for federal medical research funding.” 19 February, 2019. https://dcri.org/duke-top-10-funding/
Patient generated health data (PGHD): “PGHD can come from a wide variety of sources, said Foschini, such as devices attached to a person’s wrist or shoe, implantables, and smart devices in the home or car (Gambhir et al., 2018). In addition, there are PGHD available from social media sources, as well as data that patients report themselves such as surveys or diaries.
The growing use of wearables and mobile technologies, David Martin, associate director for Real World Analytics, FDA, said, may enhance our ability to collect patient-generated prospective data, and there are opportunities to link these data with claims or electronic health record (EHR) data.” Pg 92 2019.
Real-World Evidence Generation and Evaluation of Therapeutics: Proceedings of a Workshop (2017) National Academies of Sciences, Engineering, and Medicine. 2017. Real-World Evidence Generation and Evaluation of Therapeutics: Proceedings of a Workshop. Washington, DC: The National Academies Press. Ch 2:p 7-86. https://doi.org/10.17226/24685. https://www.nap.edu/read/24685/chapter/3
U.S. Office of Government Ethics, 5 C.F.R. part 2634. Executive Branch Personnel Public Financial Disclosure Report (OGE Form 278e), Filer: Califf, Robert. Signed 13 October, 2021. AboutbGov. https://aboutbgov.com/0Bq
















Ryan: 8-9 December 2022 NIH meeting - Gates & Fauci speaking - see Jordan Schachtel substack today for details
https://dossier.substack.com/p/bill-gates-will-join-fauci-this-week
https://www.acd.od.nih.gov/meetings.html